")
Earlier this year, New Matilda published the first in a three-part feature by editor Chris Graham, entitled Left Jab: From Heaven To Hell In The Shadow Of A Vaccine. ‘The Numbers Games’, is Part Two. It was delayed significantly (and un-ironically) due to illness. Part One focussed on Chris’ extraordinary downward health spiral, which began in September 2021, shortly after his second Covid-19 jab. It also looked at some of the successful aspects of Australia’s effort to confront the global Covid-19 pandemic. This edition looks in detail at some of the problems with our national response. Part 3 drops soon (UPDATE: Late December 2024 or early January 2025).
Fear can do amazing things to populations, and to politicians. Just ask Scott Morrison.
In February 2020, the former Australian Prime Minister had just finished bungling his way through an unprecedented summer bushfire crisis, holidaying in Hawaii as his country burned and then over-correcting on his panicked return, forcing himself on victims as he toured the nation’s fire grounds.
Obviously, Morrison paid in the polls for his hapless, atrocious performance. Almost 60 per cent of voters reported they were “dissatisfied” with the PM, and for the first time, Opposition leader Anthony Albanese passed Morrison as ‘preferred Prime Minister’. And then along came a global pandemic.
Within two months, Morrison’s polling had flipped, literally, on its head, climbing almost 20 points to 59 per cent “satisfied”. Only fear, and perhaps loathing (see ‘John Howard’ and ‘Tampa’) can unite a population behind a leader like that, regardless of how incompetent or unpopular that leader might ultimately turn out to be.
In Morrison’s case, he would leave office two years later as the most unpopular Prime Minister since records began in 1987, but not before subjecting an ungrateful nation to a roller coaster ride of truly epic proportions.
Through the first full year of the pandemic, Morrison’s numbers stayed at record highs, and by February 2021, his approval rating had climbed to a staggering 65 per cent, polling which was simply inconceivable a year earlier. Indeed, things were going so well for Morrison that rumours began to circulate Anthony Albanese might face a leadership challenge. The Liberals might even call an early election?
Alas, that was as high as Morrison would ever fly because before the month was out, his polling had started to crash, and the unravelling of his shambolic government would begin. In the background of Morrison’s rapid descent was Craig Kelly, a one-time furniture salesman for his failed family business and the member for the seat of Hughes, a middle-class electorate on the southern fringes of Sydney.
Like Morrison, Kelly was a member of the religious faction of the Liberal Party, opposing policies like same-sex marriage and action on climate change. Also like Morrison, before the pandemic struck Kelly had managed to find himself on the wrong side of the bushfire crisis, which, if you know anything about the electorate of Hughes, was deeply ironic.
Of the two dozen federal electorates in Sydney, Hughes – which includes the sprawling Royal National Park on its most southerly border – has traditionally been one of the most seriously impacted by fire. That knowledge didn’t stop Kelly from giving a now infamous train wreck interview on British television, downplaying the role of climate change in the catastrophe sweeping across the nation while his electorate literally burned.
It was unedifying stuff, but just as it had for Morrison, fear around the pandemic caused a lot of people to forget the damage Kelly had done to himself during the bushfire crisis. But unlike Morrison, where the pandemic was concerned Kelly wasn’t prepared to take the win and quietly ‘defer to the science’. Instead, he began using his social media accounts to push fringe theories on how to survive the ‘Great Plandemic’. Chief among his recommendations were claims that Hydroxychloroquine (HCQ) and Ivermectin, a horse wormer, could stop Covid-19 in its tracks, both claims which have since been utterly debunked.
All along, Morrison had tried ignoring Kelly’s increasingly strident claims, but by the end of 2020, Kelly’s posts were openly contradicting federal government advice which was, of course, informed by the nation’s most senior scientists.
Then, a year into the pandemic, and after amassing more than 100,000 followers, Kelly was finally banned from Facebook for spreading vaccine misinformation. Sensing a chink in the Liberal armour, and perhaps even a stirring of her own leadership ambitions, former deputy Labor leader, Tanya Plibersek pounced.
On the morning of February 2, 2021 Plibersek staged an impromptu press conference, and while she was lining up the Member for Hughes, who should come barrelling along the halls of the press gallery but the man himself, Mr Craig Kelly.
KELLY: You making any big announcements?
PLIBERSEK: Yes, I’m actually, I’m actually, telling them that the PM needs to stop you spreading these crazy conspiracy theories….
KELLY: Did you hear about Professor Clancy? You’ve gotta listen to our most senior immunologist Tanya, is Professor Robert Clancy (sic). Listen to him. Go and get his stuff. Read what he’s saying, and you’ll find out. And then you can come and apologise to us.
PLIBERSEK: My mum lives in your electorate and I don’t want her exposed to people who are not going to be vaccinated because of these crazy conspiracy theories that you’re spreading.
Politicians generally only play the ‘family card’ when they’re really desperate, and not usually 30 seconds into an exchange. So it’s pretty obvious Plibersek had been thinking about her ‘intervention’ for some time. And that’s deeply perplexing, because according to an Australian Institute of Health and Welfare (AIHW) study from 2017, when the pandemic hit Australia, Plibersek’s electorate had some of the worst vaccination rates in the country, a fact that must have been well known to its local member.
In 2011-12, the postcode ‘2000’ – literally, the suburb of Sydney, after which Plibersek’s electorate is named – had the equal worst vaccination rate for one-year-olds in the country (between 70 and 74 percent). The goal, for the record, is 95 percent. Even worse, for five-year-olds during the same period, the rate was below 70 per cent.
According to the AIHW, only a handful of other postcodes around the nation were able to match the appallingly low rates in Plibersek’s electorate, and it wasn’t just restricted to one suburb. The postcode 2011 – which includes Potts Point, Elizabeth Bay, Woolloomooloo and Rushcutters Bay – also recorded rates below 70 per cent. Ultimo, Chippendale, Darlington, Pyrmont, Surry Hills, Darlinghurst, Waterloo and Zetland, all wealthy inner-city suburbs in Plibersek’s electorate, recorded rates below 80 percent.
At this point, you might be wondering what the vaccination rates were for suburbs in Craig Kelly’s electorate? The short answer is ‘the equal highest rates in the country’. Right across Hughes, suburbs such as Sutherland, Kirrawee, Loftus, Kareela, Grays Point, Engadine, Heathcote, Woronora Heights, Yarrawarrah, Waterfall, Menai, Illawong, Bangor, Barden Ridge, Alfords Point, Voyager Point, Sandy Point, Pleasure Point, Wattle Grove, Holsworthy, Jannali, Como, Bonnet Bay, Oyster Bay boasted vaccination rates of 95 to 100 per cent.
Those numbers are for child vaccinations, and they’re pre-pandemic, so you might also be wondering how the subsequent Covid-19 vaccination roll-out fared? According to the Commonwealth, it mirrored the attitudes to vaccination exposed by the AIHW study. The numbers don’t neatly match – the AIHW looked specifically at federal electorates, while the Commonwealth data is broken down into Local Government Areas (local councils). But comparisons, while a little clumsy, can be made… although Plibersek probably wishes they couldn’t be.
The Local Government Area (LGA) of Sutherland Shire, which takes in the largest part of Craig Kelly’s former electorate, had the equal highest vaccination rate in the entire nation, exceeding 95 per cent of the population aged over 16.
The Sydney LGA – which takes in large chunks of Plibersek’s electorate – had the fourth worst vaccination rate in NSW at just 88 per cent, and the 375th worst in the nation, out of a possible 411.
In other words, Tanya’s mum was comparatively safe throughout the pandemic provided she stayed within Craig Kelly’s electorate, and didn’t go visit her daughter for dinner.
I mentioned earlier that Plibersek must have been aware of the criminally low vaccination rates of children in her own electorate. How do we know this? Well, the punchline is that for a two-year period in the AIHW study, Plibersek served as the Minister for Health and Medical Research… i.e. she was the single most senior person in the nation responsible for public confidence in Australia’s vaccination program.
Still, all’s fair in politics and pandemics, right? Speaking of which….
It’s all about the confidence, stupid
If you held a gun to the head of an Australian bureaucrat and demanded they create a system that, under close scrutiny, could undermine public confidence in vaccines, then they might come up with something that looks very much like what we have today. Or you could just do this.
The footage is from a federal parliamentary inquiry earlier this month, when Queensland Liberal National Party senator Gerard Rennick attempted to get a straight answer from pharmaceutical giant Pfizer about why Comirnaty, Pfizer’s Covid-19 vaccine, had been linked to widespread instances of cardiac inflammation, such as Myocarditis or Pericarditis. The phrase ‘drawing blood from a stone’ leaps to mind.
By way of very brief background, Myocarditis is an inflammation of the heart muscle, and Pericarditis an inflammation of tissue that surrounds the heart. There’s also Myopericarditis which, as the name suggests, is a combination of both. Any one of them is considered a serious condition and should get emergency attention, although once treated the result is usually complete recovery within a few days.
The reason Pfizer is under scrutiny from Senator Rennick – and he’s not alone, the company has been pursued in parliamentary inquiries all over the world – is because Comirnaty is an mRNA vaccine, and more than other Covid-19 vaccines, mRNAs have been linked to cardiac inflammation. This article from the renowned Mayo Clinic in the US explains the different types of vaccines very well, but briefly and in very simplistic terms:
- mRNA vaccines deliver a copy of a virus’ genetic code, rather than a portion of the actual virus itself. Pfizer (Comirnaty) and Moderna (Spikevax) are mRNAs;
- Vector vaccines (AstraZeneca, also known as Vaxzevria) place a modified version of the Covid-19 virus into a harmless host virus, which stimulates an immune response and causes your body to create antibodies;
- Protein subunit vaccines (Novavax) include only parts of a vaccine that best stimulate your immune system. Some people consider these types of vaccines the most safe.
mRNA technology is considered an easier way to make vaccines. It hadn’t been widely used until the pandemic came along, hence it’s considered by some to be ‘untested’ and ‘controversial’. In fact, the technology has been around since the 1960s. In the 1990s, it was used to create vaccines for Ebola – one of the deadliest viruses known to humans – but, of course, Ebola outbreaks have so far been restricted to Africa, where mostly black people live. So commercial development of mRNA technology stalled, because racism, until Covid-19 came along.
A publication like New Matilda isn’t going to resolve the debate around mRNA vaccines any time soon, but if you’re inclined, there are more cogent arguments ‘for and against’ here.
One of the things that is clear is that “mRNA and viral vector vaccines more often elicit transient mild to moderate side effects than other vaccine types”, according to a prominent Australian vaccine safety surveillance organisation. We’ll get to them a little later, but back to the Senate….
SENATOR GERARD RENNICK: Okay, so initially when the vaccine was rolled out, Myocarditis and Pericarditis wasn’t a recognised side effect. Does Pfizer understand why the vaccine causes Myocarditis and Pericarditis, and if not how then can it guarantee that it’s not also injuring other organs? And can you explain the process why the vaccine causes Myocarditis and Pericarditis?
Dr KRISHAN THIRU, PFIZER: Based on our clinical trials and pharmacovigilance data, as well as real world evidence following the distribution now of billions of doses of vaccine, we retain confidence, strong confidence, in the safety profile of the vaccine….
SENATOR RENNICK: [INTERRUPTING] Sorry Chair, point of order. I’ve asked, do you understand why it causes – I know that it’s a low risk – I’m asking do you understand why it causes Myocarditis? I want you to explain to me why it causes Myocarditis? Do you understand why it causes Myocarditis?
Dr THIRU: Pfizer is aware of very rare reports of Myocarditis and Pericarditis that have been temporarily associated with vaccination, however….
SENATOR RENNICK: [INTERRUPTING] Well, that’s still ongoing for some people.
COMMITTEE CHAIR TONY SHELDON: [INTERRUPTING] Senator Rennick, Dr Thiru should answer the question. Thank you Dr Thiru.
No prizes for guessing, Dr Thiru does not answer the question. Instead, in a scene straight out of a Yes Minister episode, he continues to simply recite from a prepared statement which has no relevance whatsoever to the question, while an increasingly exasperated Senator Rennick continues to interrupt.
In the end, Dr Thiru eventually concedes he doesn’t actually know the answer, which, frankly, is hard to believe. It seems more likely Dr Thiru just hasn’t been told what to say yet. Either way, he resolves to “take the question on notice”. The answer, I’ll guess, is some weeks or months away, if it ever arrives at all. But in the meantime, it’s worth correcting a few of the known ‘misdirections’ offered up by Dr Thiru.
Firstly, he tries to ‘share the blame’ by suggesting that ‘Pfizer is aware of very rare reports of Myocarditis and Pericarditis that have been temporarily associated with vaccination….’ In fact, cardiac inflammations, while linked to all Covid-19 vaccinations, have specifically been linked to mRNA vaccines like Pfizer (and Moderna) at much greater rates than other vaccines like AstraZeneca and Novavax. Pfizer has already admitted publicly (as has Moderna) that its vaccine causes cardiac inflammation.
Secondly, the phrase “very rare reports” is about as misleading a statement you can make without actually telling a bald-faced lie. We’ll come back to why shortly. In the interim, New Matilda contacted Pfizer to offer Dr Thiru the opportunity to answer the questions he clearly dodged. As you might have guessed, our emails were ignored. We did, however, receive a response from the Commonwealth government to a pile of questions about its response to Covid-19. The spin doctors from the federal Department of Health and Aged Care (DoHAC) appear to have taken a leaf out of Dr Thiru’s book.
Singapore vs Australia: who got it right?
In May 2021, a full four months before I got my second Pfizer jab, the Singaporean Government issued a public warning that citizens should “avoid strenuous exercise” for 12 to 24 hours after a Covid-19 vaccination. Singapore, if you hadn’t heard, was widely considered to be a leading nation in its response to the pandemic. At one point, it had the lowest Case Fatality Rate (CFR) of all ‘very highly developed’ nations on earth, at 290 deaths per million.
By June 11, Singapore had expanded that advice to avoid exercise for a full week, and by September – the month I happened to get my second Pfizer jab – Singapore was recommending no strenuous exercise for two weeks after the jab.
“As a precautionary measure, all individuals, especially adolescents and men below 30 years of age, who have received any dose of the COVID-19 vaccine, are advised to avoid strenuous physical activities such as running, weightlifting, competitive sports, or playing ball games for two weeks after the vaccination.”
I’m no adolescent, nor am I under 30. But at 49, I was a pretty fit, active guy. To recap briefly, two days after my second Pfizer shot, I went out for a surf – like I did every other day – and got into quite a bit of trouble. You can read more about that here, in Part 1 of this feature. Within six weeks I was being airlifted to a Brisbane hospital, and in the year and a bit since, as I’ve checked in and out of hospitals in two states and one territory, I’ve started to wonder more and more about that health warning from Singapore.
Specifically, I’ve wondered why they saw the need to issue it, and Australia didn’t? A journalist in New Zealand has wondered the same thing, noting that while no official notice came from the NZ Government, individual doctors were issuing advice against strenuous exercise after vaccination. I’ve heard the same anecdotal information regarding many Australian GPs. So I went to the federal Department of Health and Aged Care (DoHAC), and asked them: “Does the TGA have any comment on why the Singaporean Government issued a warning against vigorous exercise after a Covid-19 vaccine, but Australia did not issue this advice?”
It’s a pretty simple question… which DoHAC promptly ignored. Rather than explain why that advice wasn’t issued in Australia, DoHAC instead explained who made the decision, which, if you were of suspicious mind, kind of looks like them pre-emptively throwing someone else under a bus:
“The Australian Technical Advisory Group on Immunisation (ATAGI) advises the Minister for Health and Aged Care on the National Immunisation Program (NIP) and other immunisation issues. This includes clinical advice to medical practitioners and patients on how to administer and manage immunisation in clinical practice. ATAGI has developed specific guidance on Myocarditis and Pericarditis after COVID-19 vaccines, including advice on exercise. This guidance was produced with the Cardiac Society of Australia and New Zealand (CSANZ), the Royal Australian College of General Practitioners (RACGP), the Australian College of Rural and Remote Medicine (ACRRM), the Australasian College for Emergency Medicine (ACEM) and the Paediatric Research in Emergency Departments International Collaborative (PREDICT).”
In other words, ‘We don’t know why Singapore issued that advice and Australia didn’t…’ or possibly, ‘We do know why, and we’re not going to tell you’. Either way, we still don’t know the answer to why Singapore advised citizens not to exercise, and Australia didn’t. But we do know this: someone is almost certainly going to turn out to be wrong, and I have a feeling in my bones it’s not going to be Singapore.
I also know this: when a government agency so blatantly ignores a simple question, there’s usually a reason for that. So I’ll either wait for a leak (‘deepthroats’ can contact me via Signal or Telegram on 0407 555 328), or I’ll slip some questions to a friendly politician for the next Senate hearing (Senator Rennick, expect a call sometime soon).
In the meantime, there’s some other ‘conflicts between nations’ – or rather, conflicting approaches to the pandemic – that warrant closer inspection.
Canada vs Australia: who got it right, eh?
By early 2021, a year after the pandemic started, Australia was poised to begin rolling out our national immunisation program. Our first planeload of Pfizer vaccines – 142,000 doses in all – touched down in Sydney on February 15. Coincidentally, they made it here via a Singapore Airlines flight.
One week later, people were getting jabbed, including Scott Morrison, whose standing in the polls had just started to head south.
Around the same time, the Delta variant of Covid-19 was starting to take hold, so there was growing pressure on health authorities to get vaccines into arms as quickly as possible. One of the measures they adopted to speed things up was to reduce the gap between first and second doses for the AstraZeneca vaccine, from 12 weeks to between four to eight weeks. This was also around the time AstraZeneca was developing an increasingly bad reputation, after several early deaths were directly linked to the vaccine.
I remember wondering at the time, what might that haste actually cost us? Is it safe to get two jabs closer together? Surely, if the ideal time is three months apart, then it’s better to wait? But obviously, there’s a reason I don’t serve on the Australian Technical Advisory Group on Immunisations (ATAGI) which made the call… I’m not an expert on immunisations.
I also remember feeling that the growing criticism of Morrison and the Commonwealth was a bit harsh. My thinking was partly influenced by the fact this was a pandemic – a first for everyone – and that the only certainty was things were going to go wrong. But my view was mostly influenced by what New Matilda’s Geoff Russell wrote about how poorer countries without the buying power of their richer neighbours might access vaccines.
Geoff argued that if wealthy nations gobbled up all the vaccines as quickly as possible, deaths in poorer nations would be even higher.
“The Economist this week had a special feature on the impact of the virus in poor countries; they noted that Uganda had more cabinet ministers than ICU beds. We don’t only have to halt this virus for our own benefit, but for everybody’s. We really are all in this together.”
Apparently, Justin Trudeau, the Prime Minister of Canada, doesn’t read Geoff Russell or New Matilda, because it subsequently emerged that his ‘left-wing’ government experienced what Australians did when it came to toilet paper: panic-buying. By the end of 2020, Trudeau had signed seven different contractual arrangements for vaccines, and in the process secured Canada up to 414 million vaccine doses… for a population of just 38 million. In other words, screw the world’s poor.
Ironically, in one of those ‘you got what you deserved’ moments that you generally only see in Hollywood films, by early 2021, Canada found itself trailing most of the rest of the first world’s vaccination rollout. Very badly. In fact, they were doing even worse than Australia was, and that’s because in trying to gobble up all the vaccines he could find, Trudeau had been forced to order from Europe, not his neighbours in the United States. And that’s because US president Donald Trump was engaged in the same game of political populism as Trudeau, with threats to ban vaccine exports under his ‘America First’ policy.
Europe, to a lesser extent, did the same thing by prioritising its own citizens, and so Canada found itself stuck with a huge back order of vaccines that it couldn’t fill, and mostly wouldn’t need.
In the end, it meant that while nations like Australia were reducing the time gap between first and second doses with AstraZeneca, over in Canada they were increasing the time gap for two Pfizer shots, from three weeks to a whopping four months, more than five times the gap recommended by the Pfizer clinical trials. Canada’s National Advisory Committee on Immunisation (NACI) explained:
“… In the context of limited COVID-19 vaccine supply, jurisdictions should maximize the number of individuals benefiting from the first dose of vaccine by extending the interval for the second dose of vaccine up to four months. [This creates] opportunities for protection of the entire adult population within a short timeframe… [and will also]contribute to health equity.”
In laymen’s terms, Canada’s strategy was to get ‘less of the vaccine’ in more arms, thus providing a greater proportion of the population at least some protection. But there’s a twist, and it’s the sort of thing you never see in Hollywood films.

According to the Association of American Medical Colleges, Canada’s initial greed turned out to be a ‘stroke of good fortune’. Not only did the gap between doses increase the effectiveness of the Pfizer vaccine by stimulating a stronger immune response, but according to a study subsequently published on medRxiv, the further apart the first and second doses of mRNA vaccines were administered, the lower the rate of injury.
“Overall reporting rates were higher when the inter-dose interval was shorter (less than 30 days) for both vaccine products,” the report discovered.
Injury, in particular cardiac inflammation, was found to be significantly higher after the second dose, so waiting longer between doses gave the body time to adjust.
And there you have it: in seeking to ingratiate himself with Canadian voters by screwing over the rest of the world, Justin Trudeau had actually protected them from greater harm. Although harm is all relative, of course. Because the same study also found this:
“The highest reporting rate of Myocarditis/pericarditis was observed in males aged 18-24 years following [Moderna] as the second dose; the rate in this age group was 5.1 times higher than the rate following [Pfizer] as the second dose.”
In other words, mRNA vaccines, in particular Moderna, caused the highest rates of cardiac inflammation in the people least likely to suffer harm from Covid-19 itself. Although that’s not what you would have come to understand if you relied on the spin put out by Big Pharma and government officials, particularly in Australia.
Rare is in the eye of the beholder
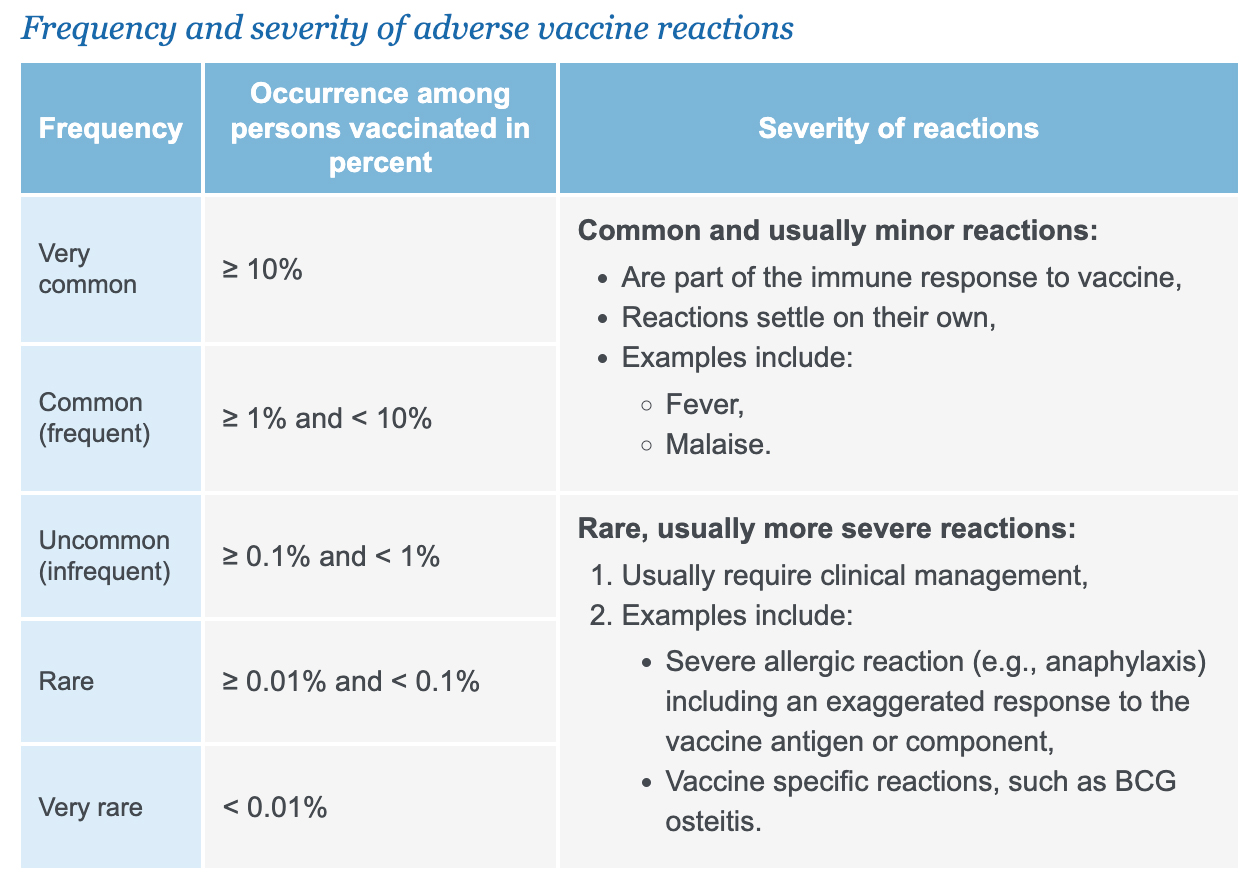
Pharmaceutical companies, media outlets and governments around the world have been at pains to point out that dangerous reactions to the Covid-19 vaccines – also known as ‘Adverse Events Following Immunisation (AEFIs)’ – are ‘rare’ or ‘very rare’. What they don’t tell you is what ‘rare’ or ‘very rare’ actually means, numerically speaking.
Helpfully, the United Nation’s World Health Organisation (WHO) does. A chart which outlines the categories reveals that any adverse event – and that can include anything from headache or a sore arm where you got the jab, all the way to anaphylaxis or death – occurring at a rate of greater than ‘one in 1,000’ is considered ‘rare’; and anything occurring at greater than ‘one in 10,000’ is considered ‘very rare’.
Or course, like beauty, the perception of what is and isn’t ‘rare’ or ‘very rare’ is in the eye of the beholder. And to no small degree, it depends on what you’re being asked to do or accept. If I told you that out of 1001 planes sitting on a tarmac, one of them was going to crash and burn, now pick which one you want to fly in, you’d probably choose to drive instead. Suddenly, ‘one in 1001’ doesn’t seem so rare.
Of course, during the pandemic, Australians weren’t being asked to choose between a ‘one in 1001’ chance of life or death. For most of us, we were being asked to choose between the risk of an ‘adverse event’, most of which were extremely mild, and a virus, which had a reasonably good chance of making us very sick.
Ordinarily, that would feel like a pretty simple choice, and traditionally high vaccination rates in Australia suggest it is. But problems start when governments spin data to try and strengthen public confidence. Like the federal government did when I emailed them a pile of questions earlier this year about incidences of cardiac inflammation after Covid-19 vaccination (you can read all the questions from New Matilda, and the government’s response, here).
DoHAC’s answers were consistent with information already promoted throughout the pandemic, including daily Covid-19 vaccine safety reports from the Therapeutic Goods Administration (TGA), the government agency that oversees vaccine distribution and safety in Australia:
“Myocarditis and Pericarditis (inflammation of the heart or membrane around the heart) are known but very rare side effects of COVID-19 vaccination. Myocarditis is reported in around 1-2 in every 100,000 people who receive Comirnaty (Pfizer) and around 2 in every 100,000 of those who receive Spikevax (Moderna).”
The emphasis is mine, because while the claims are technically correct, they’re also deeply misleading, which is exactly what they were calculated to be, and how they got there is a master class in spin.
Firstly, isolate the figures to one condition, for example ‘Myocarditis’. Don’t mention Myopericarditis or Pericarditis, the latter of which had a reporting rate three times that of Myocarditis. And whatever you do, don’t give a figure for ‘cardiac inflammation’, which, while obviously more accurate and relevant would reveal a considerably higher number of injuries.
Secondly, talk about ‘doses’, not actual people. You can do this by only providing figures for adverse events associated with the second dose of the vaccine. Don’t mention figures for the first dose as well, in other words, don’t combine the figures for the first and second doses. And don’t even think about including figures from third, fourth etc doses. This avoids giving a ‘total number of people injured by the vaccine’, and limits the number to a much more narrow band.
Thirdly, and most importantly, quote figures from across the entire Australian population, rather than specific age groups.
For example, while it’s true to say ‘Myocarditis is reported in around 1-2 in every 100,000 people who received an mRNA vaccine’ it’s also correct to say that boys aged 12 to 17 years who received an mRNA vaccine experienced cardiac inflammation in about one in every 4,200 cases. That’s one hell of a long way from ‘1-2 in every 100,000’. And it still only relates to one condition (just Myocarditis, not Pericarditis as well) and one dose (the second).
It’s also true that men aged 18 to 29 may have experienced cardiac inflammation at rates of about one in 3,333. And in all likelihood, even those rates are grossly understated, and we’ll come to why in a minute, because as alarming as the real numbers are, it would be unfair not to emphasize that while authorities acknowledge cardiac inflammation is no trifling matter, “cases are usually mild and resolve within a few days”.
So said DoHAC, who added that the TGA was “carefully monitoring and reviewing reports of these adverse events and publishes fortnightly updates in the COVID-19 vaccine safety report. ATAGI continues to emphasise that the protective benefits of the mRNA vaccines far outweigh the rare risk of these side effects”.
Notably, this study published in 2021 found that the risk of people aged under 20 developing Myocarditis from an actual Covid-19 infection was more than twice that of the known risk from vaccination: in males aged 16-19 it was as high as one in 1,666, which is getting close to ‘uncommon’, rather than the ubiquitous and far less scary ‘rare’.
That argument however, is seriously undermined by the reality that the vaccines largely didn’t prevent transmission or contraction of Covid-19. So, risking cardiac inflammation from vaccination to remove or significantly reduce the risk of cardiac inflammation from the disease itself is a moot point, because you’re basically risking cardiac inflammation twice.
Of course, vaccines weren’t aimed at just preventing cardiac inflammation, and they did, undeniably, make people who subsequently got the disease less sick. But to add literal insult to injury, even the ‘bad’ vaccination figures which reflect high rates of injury don’t tell the full story.
Bring out your dead
Believe it or not, there’s no universal agreement on how best to monitor vaccine injury across Australia. Known as an ‘Adverse Event Following Immunisation (AEFI)’, it is mandatory for health providers in NSW, Western Australia, Queensland, Northern Territory and the ACT to notify authorities if they believe a vaccine or medicine may have caused harm. It is not mandatory in South Australia, Victoria and Tasmania.
Ostensibly to plug that gap, in 2012 the Commonwealth set up a public website where everyone – health officials, pharmaceutical companies, and especially members of the public – could report their suspicions around vaccine and medicine injury. Called the Database of Adverse Event Notifications (DAEN), entries are de-identified and then released to the public in a searchable database 14 days after they’re “accepted” by health officials.
The DAEN has been relied on by pharmaceutical companies, health authorities and successive federal governments as a key component in the ongoing effort to promote public confidence in vaccine safety. But in truth, the data collected by the website is complete rubbish, a reality the TGA all but acknowledges with a caveat on its website.
“We encourage people to report even if there is only a very small chance that a medicine was the cause. These reports are entered into the database without being confirmed or assessed to determine if they are caused by a medicine. Many of the reports are made voluntarily and may be incomplete or inaccurate.”
That’s somewhat of an understatement. But let’s have a look at the numbers regardless, before we delve into the detail, which on this occasion is where the devil is hanging out.
Pre-pandemic, in a ‘good’ year, the DAEN might get about 21,000 or so reports of ‘adverse events’ where medicines or vaccines are suspected as the cause. But in 2021, after the Covid-19 vaccines arrived in Australia, reporting exploded.
The DAEN is what’s known as a ‘passive’ vaccine surveillance system because, in effect, the federal government is 'passively' relying on you, the public (along with doctors, nurses, health workers etc) to come to them and tell them ‘what happened’. You can probably guess how that might go, particularly amidst the panic of a pandemic.
In the first six months of the vaccine roll-out – February to August 2021 – the DAEN received 2,316 reports from ‘chest pain’ after vaccination was listed as the adverse event. Over the same period, there were 1,208 reports of ‘palpitations’; 977 reports of ‘tachycardia’ (which means a rapid heartbeat); 875 reports of Hypertension (high blood pressure); 113 reports of ‘Troponin increased’ (which suggests a cardiac problem); and 295 cases of ‘Hypotension’ (low blood pressure).
At the same time, there was 1,154 reports of ‘chest discomfort’, which sounds an awful lot like ‘chest pain’; 423 reports of ‘heart rate increased’ (another way of saying ‘Tachycardia’); 508 reports of ‘blood pressure increased’ (also known as ‘Hypertension’); 99 cases of ‘blood pressure decreased’, aka ‘Hypotension’; and at least five additional listings describing ‘Troponin’ in various ways. There were separate listings for heart murmurs; for heart flutters; for heart attacks; for Myocardial infarctions; for Atrial fibrillation; for Bradycardia and slow heart beats; and it goes on, and on and on, with almost 4,000 separate entries.
You can probably see where this is heading: the repetition in the DAEN almost beggars belief, to the point where it renders the data absolutely worthless. It’s basically a free-for-all when it comes to naming adverse events.
That appears to be how 15 people came up with “hangover” as an adverse event. While it may ultimately transpire that Covid-19 vaccines are bad for your heart, they almost certainly shouldn’t get you drunk. Having said that, so far 32 people have reported that’s how they felt after their vaccination. Another 33 revealed their jabs caused an adverse event known as “crying”, and 14 reported “hunger”, one of whom claims to have died shortly thereafter.
One person listed “moaning” as their adverse event, but on the upside, another reported their “exercise tolerance increased” (somebody should let the World Doping Agency know that Covid-19 vaccines can knock time off your 100-metre sprint).
One of the more puzzling entries was “drowning”, which, curiously, was not listed as a case where “death was a reported outcome”. But by far my favourite entry was a claim that the Pfizer vaccine gave someone “Genital herpes zoster”, which sounds a bit like Mary trying to explain to Joseph how the Virgin birth came about. Or in this case, ‘I swear to God honey, I got genital herpes from the Covid-19 vaccine….’
It’s also a free for all when it comes to categorising adverse events. As you might expect, many of the cardiac issues that arose were listed under the category ‘Cardiac disorders’. But tens of thousands were listed under other categories, including ‘vascular disorders’, ‘general disorders and administration site conditions’, and ‘Investigations’. Under the category ‘Injury’ you’ll find almost 800 pointless entries for ‘Adverse event following immunisation’… on a database set up specifically to register ‘Adverse Events Following Immunisation’.
The practical effect of this kind of ‘Choose your own adventure/medical condition’ is that anyone seeking to inform themselves about the safety of a vaccine – which is why the DAEN purports to be publicly available in the first place – needs a degree in mathematics to make any sense of it, before they quickly realize that no-one, not even someone with a degree in mathematics, could ever make any sense of it.
The information in the form its presented to the public is not only worthless, but leaves itself open to abuse by individuals and groups seeking to undermine public confidence in Australia’s immunisation program (more on them in Part 3 of this special series).
Speaking of confidence…
What the Database of Adverse Event Notifications lacks in quality, it absolutely does not make up for in quantity. According to a February 2021 paper published in Australian Prescriber, “Probably less than 5% of adverse reactions are reported, even in countries where reporting is mandatory.” And just a reminder, Australia is not a country where reporting is mandatory in all jurisdictions.
Luckily, in addition to our ‘passive’system, Australia also has an ‘active’ vaccine safety surveillance system running alongside the DAEN. It’s run by AusVaxSafety, a government-funded non-profit run out of the National Centre for Immunisation Research and Surveillance.
During the pandemic, AusVaxSafety reached out directly via email and phone to Australians who’d been vaccinated, almost five million of them in the first six months of the vaccine roll-out (February 22 to August 31, 2021). 3,035,983 of them responded.
As AusVaxSafety itself acknowledges, there’s likely to be a bias towards people who suffered an adverse event: “People experiencing AEFI may be more motivated to respond, inflating the apparent frequency of AEFI. Conversely, those with severe AEFI may be less able to respond.”
However it comes out in the wash, a survey that motivates just over three million people to share their recent vaccination experience is, by any reckoning, a massive sample size, and an impressive feat.
Here’s what AusVaxSafety found: “… 35.9% of respondents reported one or more AEFI… up to three days after the first Comirnaty dose; 54.7 per cent after the second Comirnaty dose; 52.8 per cent after the first Vaxzevria dose; and 22 per cent after the second Vaxzevria dose.”
So what does that mean in raw numbers? 1,300,162 people reported an adverse event shortly after receiving a COVID-19 vaccine. It’s important to acknowledge what those adverse events mostly were: “Local pain, fatigue, headache, and myalgia were the most frequently reported symptoms.”
So they were mild adverse events. But equally, it’s ridiculous to think that if the level of mild reactions increases exponentially the more you ask people, the level of more serious reactions won’t also increase, even if its likely to increase at gentler rate.
Over the same period of time, the ‘passive’ DAEN system logged 60,780 events, a tiny percentage of what the active surveillance system found. And bear in mind, the AusVaxSafety numbers only cover the first six months of the roll-out, a period when less than one-third of the Australian population had been vaccinated, and they only reached about 25 per cent of the estimated number of people vaccinated.
Now here’s the rub: 28,298 of those people – almost ‘one in every 100’ surveyed, and more than 'one in 50' who reported an adverse event - were so unwell they required ‘medical review’ within three days of vaccination. Of those people, 17,065 returned to their doctor, and 5,107 ended up presenting to hospital.
As shocking as that might sound, when you boil it all down, vaccine safety really is just a numbers game. In crude terms, it’s about how many people you can save, versus how many you harm along the way. Big Pharma calls it the ‘benefit-risk ratio’, although politicians tend to view it more like ‘what you can get away with’.
If you’re Scott Morrison, numbers are about polling and how popular you are. Or if you’re Tanya Plibersek, they're about trying to make someone else’s electorate look more dangerous than yours. For Craig Kelly, numbers can help you make crackpot ‘cures’ look safer than they really are. And if you’re a large government department charged with safeguarding public confidence in our health system, then numbers might be useful to convince a journalist that ‘only about 1-2 in every 100,000 people’ developed Myocarditis after an mRNA vaccine.
From my perspective, numbers are much more personal, because if you’d told me way back in September 2021, just before I had my second Pfizer jab, that ‘about 1-2 in every 100 responders’ to a massive vaccine safety survey would need to seek medical help within three days of receiving their second dose of Pfizer, well, I’m not so sure I’d have agreed to take it.
And if you’d told me that of those people, about one in every eight of them would end up in a hospital emergency department, just like I did, well….
See what I did there?
Part 3 – the final edition of this special investigation - will be published in New Matilda in late December 2023-early January 2024. In the meantime, you can support Chris' work, and that of New Matilda, by making a one-off contribution here, or by subscribing here.
Donate To New Matilda
New Matilda is a small, independent media outlet. We survive through reader contributions, and never losing a lawsuit. If you got something from this article, giving something back helps us to continue speaking truth to power. Every little bit counts.

")
 In World FAFO Championships")
{kind=link}