Last week, Ben Eltham summarised the Grattan Institute’s recent work on budget pressures on Australian governments, projecting a $60 billion gap between public revenue and public spending over the next 10 years – a gap which, contrary to some perceptions, could be higher under a Coalition than a Labor Government.
While that gap is well below European or American proportions, it does draw attention to one particular area of public finance – health expenditure. Two thirds, or $40 billion, results from growing health expenditure.
The risk we face is not that government health expenditure will break the bank, but that the policy response from future governments will focus only on immediate fiscal costs, at the expense of higher community costs and greater inequity in access to health care.
The simplest path to bad policy like this is to shift health costs “off budget” and, through a combination of incentives and compulsions, on to private health insurance (PHI). Lobbyists for private health insurers make the glib and superficially plausible argument that PHI is the obvious means to make this saving through mechanisms like “Medicare Select”, a system which would essentially destroy Medicare and conscript Australians into PHI.
The false logic of such self-interest needs clarifying.
Shifting costs from public spending to private spending is not a saving. We are no better off if we save a dollar in taxes only to have to spend a dollar in the private sector, without any better outcome. In fact, because of the high administrative overhead of PHI, the figure is more like an outlay of $1.10 to save $1.00 in taxes, but we have been conditioned to believe that while public bureaucracy is bad, private bureaucracy is virtuous.
PHI is essentially a “privatised tax”, collected by NIB, HCF or Medibank Private, rather than the Australian Taxation Office, to fund our shared health care needs. We may not relish paying taxes, but we have to admit that the Australian Taxation Office does a fairer and more efficient job at collecting tax than private financial agencies.
Worse, because of its demonstrated incapacity to control service providers’ costs, combined with a tendency for consumers to over-spend on health insurance, PHI results in high over-use and over-charging, a situation most clearly manifest in the USA where health care costs are now 18 per cent of GDP, compared with our 9 per cent. Nine percent of GDP is enough to fund Gonski, a national disability scheme and a fast train, with a little left over for tax cuts or some ships for the navy. Private health insurance, as a permissive funding channel, makes health care more expensive, but it doesn’t buy better care or produce better outcomes.
A more sensible policy response than cost-shifting is to raise taxes to cover increasing health outlays, making sure that no one feels any need to waste their money on PHI. After all, more than 80 per cent of Australians would like to see more government spending on health care and our taxes are very low in comparison with other prosperous countries.
Such a policy, while more equitable and economically responsible than delegating health expenditure to PHI, however, is only partial, for it does not necessarily address the underlying supply-side and demand-side drivers of health care.
To its credit, the Commonwealth Government has been focusing on supply-side cost issues: since 2000 price inflation in health care has been about one per cent lower than general price inflation. There has been a long-standing commitment by the Commonwealth to use its bargaining power to keep pharmaceutical prices under control, and both Coalition and Labor governments have tried to contain public hospital costs – Coalition governments through stringency in state hospital grants and Labor governments through conditionality in those grants.
There are undoubtedly more cost savings to be made, particularly in terms of structural reform of health care, which in many aspects still operates along cottage industry lines and which has little integration across different areas of care – hospital, medical and pharmaceutical services, and which has an almost complete separation between public and private hospitals.
Where expenditure has grown however, and will continue to grow, is in utilisation. Over the 27 years of Medicare records, from 1984-85 to 2011-12, per capita utilisation of Medicare services has doubled. We may believe that this is a normal outcome of ageing, but it has occurred across all age groups, as indicated in the graph below, compiled from Medicare data.
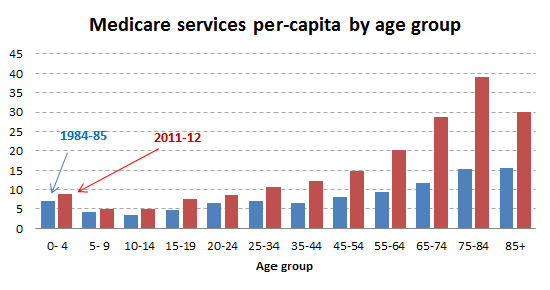
Some of this growth results from new Medicare items being added to the schedule, but for the most part it is about more use of health services. Note, in particular, the high growth among the 35 to 64 age groups.
There are many competing explanations for this growth. Some attribute it to the “moral hazard” of services which are free at the point of delivery, thus encouraging overuse – a problem, incidentally, that PHI shares with Medicare. (The right complain about the “nanny state” while promoting the “nanny corporation” in its place.)
There are new therapies. There are improved diagnostic techniques allowing for previously undetected conditions to be detected and treated. Some conditions, which once led to a rapid death, allow people to live on, thereby using more care. There has been a huge growth in obesity leading to lifestyle-related disease. Risk-aversion by health care providers fearing lawsuits meshes with increased consumer expectations of cures. Many social commentators point to the interrelationship of poverty, inequality, social exclusion and poor health, while others point to the concentration of demand for health services among people with multiple dysfunctional conditions, such as overuse of alcohol and other drugs, gambling addiction and minor criminal behaviour.
What this all indicates is that health care is a complex system, which needs to be managed as a system through the strong hand of government. So long as governments remain under fiscal pressure, and so long as they do not succumb to the temptation to shift health care costs off-budget, they have an incentive to find which therapies and other interventions work and which do not, and to make appropriate policy responses – through controls on providers, judicious use of prices (including means-testing), persuasion, taxation, and use of broader policies to do with social conditions with health consequences. In short, they have a fiscal incentive to see that money is spent wisely.
This contrasts with the view of those in the private sector who see health care as a potential goldmine, if only it can be unleashed from the tight hand of government control – a view captured so well in the title of a keynote address of a health insurers’ conference scheduled for July: “Government cutbacks – a sea of opportunity.”
We should be wary about the PHI industry. It has always been given a privileged position by Coalition governments, and the current Gillard Government, unlike previous Labor governments, has allowed PHI coverage to rise from 43 to 47 per cent of the population. It is extraordinary that when we have just witnessed the harm the financial sector can inflict on the real economy, we have given this branch of the financial services industry such a privileged position. We need to see PHI for what it is – an industry with a high bureaucratic overhead and with every incentive to see its market expand – rather than as part of our health care system.
Donate To New Matilda
New Matilda is a small, independent media outlet. We survive through reader contributions, and never losing a lawsuit. If you got something from this article, giving something back helps us to continue speaking truth to power. Every little bit counts.


